
Congenital coronary artery anomalies
Citation, DOI, disclosures and article data
At the time the article was created The Radswiki had no recorded disclosures.
View The Radswiki's current disclosuresAt the time the article was last revised Liz Silverstone had no financial relationships to ineligible companies to disclose.
View Liz Silverstone's current disclosures- Congenital coronary artery anomaly
- Congenital coronary arterial anomalies
- Congenital coronary artery anomalies (CCAA)
- CCAA
- Congenital coronary artery abnormality
- Congenital coronary artery abnormalities
- Congenital coronary arterial abnormalities
- Coronary artery anomalies (CAAs)
- Coronary artery anomalies
- Coronary artery anomaly
- Congenital anomaly of the coronary arteries
- Coronary artery variants
- Coronary artery variant
Congenital coronary artery anomalies (CCAAs) are not common, found only in ~1% (range 0.1-2%) of patients 1,3.
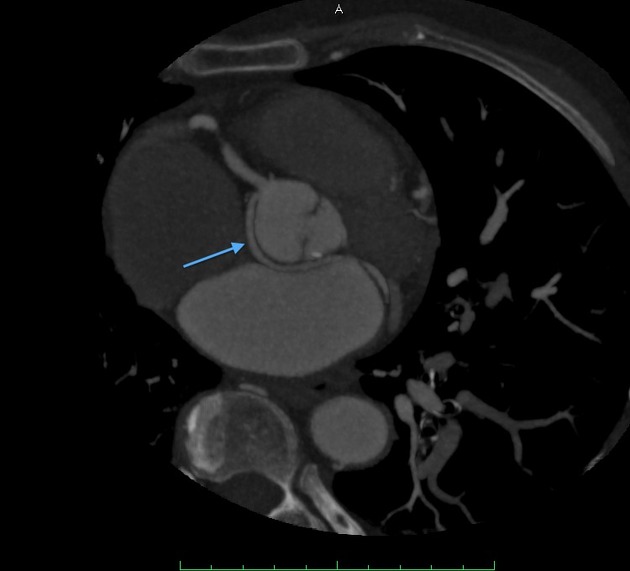
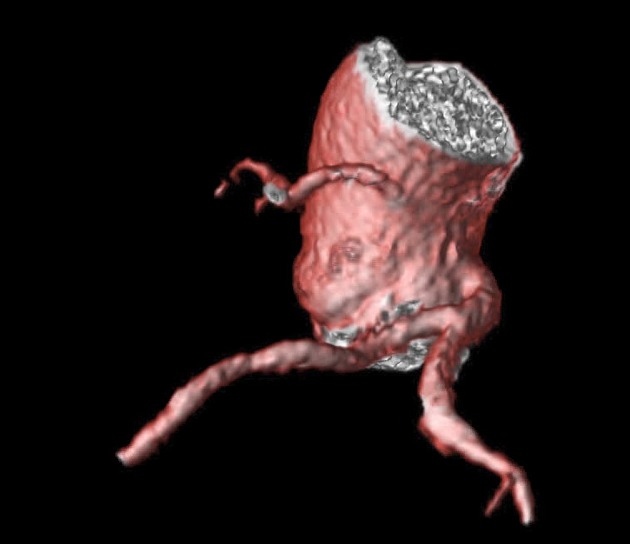
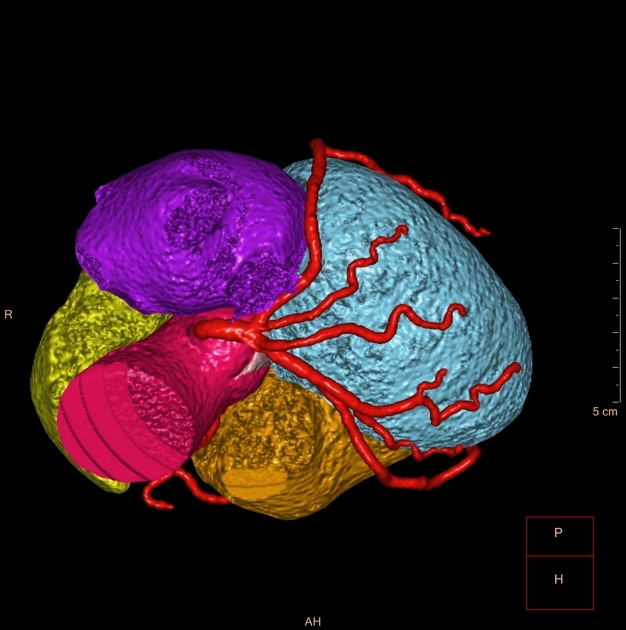
The major anomalies are due to abnormal course, abnormal origin or a combination of both.
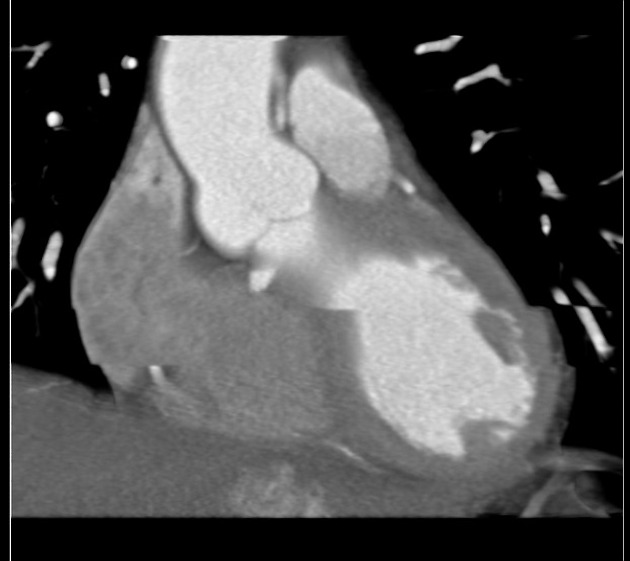
The most important finding to look for is the "malignant" course of the anomalous coronary artery, i.e. does the artery run between big pulsating objects - right ventricular outflow tract / pulmonary artery on one side and aorta on the other? Increased pulsations during or following exercise can sometimes compress the coronary artery enough to diminish blood flow to the myocardium, which can cause a re-entry phenomenon in the myocardium and sudden cardiac death due to ventricular fibrillation or sustained ventricular tachycardia.
Interarterial "malignant" course is most commonly identified in the right coronary artery, classically presenting in young adults or teenagers with sudden cardiac death. It is estimated that around a quarter of sudden cardiac deaths in this population are caused by malignant coronary artery course.
An intramural course of a coronary artery (known as myocardial bridging) is another lesion which may be hemodynamically significant and present with exertional angina. Usually, it occurs at mid-LAD. It is important to describe the location (LAD segment relative to branch vessels), length, and depth of bridging in your report.
Of course, all anomalous coronary artery anatomy should be described in the radiology report, as this may be used to guide catheter angiography by the interventional cardiologist 7.
Related pathology
A vast number of different coronary artery abnormalities have been described and are discussed separately (see related articles).
Variant anatomy is described in each of the separate vessel articles and can be group into variants of origin, course, branching, and distribution.
References
- 1. Datta J, White C, Gilkeson R et al. Anomalous Coronary Arteries in Adults: Depiction at Multi-Detector Row CT Angiography. Radiology. 2005;235(3):812-8. doi:10.1148/radiol.2353040314 - Pubmed
- 2. Dodd J, Ferencik M, Liberthson R et al. Congenital Anomalies of Coronary Artery Origin in Adults: 64-MDCT Appearance. AJR Am J Roentgenol. 2007;188(2):W138-46. doi:10.2214/AJR.05.2098 - Pubmed
- 3. Pelliccia A. Congenital Coronary Artery Anomalies in Young Patients: New Perspectives for Timely Identification. J Am Coll Cardiol. 2001;37(2):598-600. doi:10.1016/s0735-1097(00)01122-0 - Pubmed
- 4. Angelini P. Coronary Artery Anomalies: An Entity in Search of an Identity. Circulation. 2007;115(10):1296-305. doi:10.1161/CIRCULATIONAHA.106.618082 - Pubmed
- 5. Shriki J, Shinbane J, Rashid M et al. Identifying, Characterizing, and Classifying Congenital Anomalies of the Coronary Arteries. Radiographics. 2012;32(2):453-68. doi:10.1148/rg.322115097 - Pubmed
- 6. Kim S, Seo J, Do K et al. Coronary Artery Anomalies: Classification and ECG-Gated Multi-Detector Row CT Findings with Angiographic Correlation. Radiographics. 2006;26(2):317-33; discussion 333. doi:10.1148/rg.262055068 - Pubmed
- 7. Young P, Gerber T, Williamson E, Julsrud P, Herfkens R. Cardiac Imaging: Part 2, Normal, Variant, and Anomalous Configurations of the Coronary Vasculature. AJR Am J Roentgenol. 2011;197(4):816-26. doi:10.2214/ajr.10.7249 - Pubmed
- 8. Sundaram B, Patel S, Bogot N et-al. Anatomy and terminology for the interpretation and reporting of cardiac MDCT: part 1, Structured report, coronary calcium screening, and coronary artery anatomy. AJR Am J Roentgenol. 2009;192 (3): 574-83. doi:10.2214/AJR.08.1177 - Pubmed citation
- 9. Sundaram B, Patel S, Bogot N, Kazerooni E. Anatomy and Terminology for the Interpretation and Reporting of Cardiac MDCT: Part 1, Structured Report, Coronary Calcium Screening, and Coronary Artery Anatomy. AJR Am J Roentgenol. 2009;192(3):574-83. doi:10.2214/AJR.08.1177 - Pubmed
- 10. Hauser M. Congenital Anomalies of the Coronary Arteries. Heart. 2005;91(9):1240-5. doi:10.1136/hrt.2004.057299 - Pubmed
- 11. Rahalkar A & Rahalkar M. Pictorial Essay: Coronary Artery Variants and Anomalies. Indian J Radiol Imaging. 2009;19(1):49-53. doi:10.4103/0971-3026.45345 - Pubmed
- 12. Villa A, Sammut E, Nair A, Rajani R, Bonamini R, Chiribiri A. Coronary Artery Anomalies Overview: The Normal and the Abnormal. World J Radiol. 2016;8(6):537-55. doi:10.4329/wjr.v8.i6.537 - Pubmed
Incoming Links
- Ischaemic cardiomyopathy
- Hypoplastic circumflex artery
- Coronary CT angiography (protocol)
- LCx and LAD arising separately from the left aortic sinus
- Coronary ostial dimple
- Myocardial ischaemia
- Tetralogy of Fallot
- Anomalous aortic origin of coronary artery
- Coronary Artery Disease - Reporting and Data System
- Coronary arteriovenous fistula
- Prepulmonic coronary course
- Hypoplastic right coronary artery
- Transseptal coronary course
- Right coronary artery
- Sudden cardiac death
- Hypoplastic left anterior descending artery
- Anomalous course of coronary arteries
- Coronary arteries
- Cardiac CT (an approach)
- Myocardial bridging of the coronary arteries
- Anomalous left coronary artery origin with septal (subpulmonic) course
- Anomalous right coronary artery from the pulmonary artery (ARCAPA) with coronary artery ectasia
- Left coronary artery anomaly
- Single coronary artery - right
- Anomalous origin of the left coronary artery with malignant course
- Double outlet right ventricle, malposition of the great vessels and pulmonary hypoplasia - treated with Rastelli procedure
- Anomalous left coronary artery from the pulmonary artery (ALCAPA)
- Anomalous origin of left circumflex artery from right coronary sinus
- Complex congenital fistula between the coronary, bronchial and pulmonary arteries
- Aberrant left main coronary artery
- Tubular origin of right coronary artery
- Left main to coronary sinus fistula
- Congenital atresia of the right coronary artery ostium
- Separate left anterior descending artery and left circumflex artery origins
- Separate LCx and LAD origins from left coronary cusp
- Anomalous origin of the circumflex artery with retro-aortic course
- Single coronary artery
- Anomalous left main coronary arterial origin
- Anomalous right coronary artery (ARCA) with interarterial course
Related articles: Pathology: Vascular: Congenital coronary artery anomalies
-
congenital coronary artery anomalies
- absent coronary artery
- absent circumflex artery
- absent right coronary artery
- absent left anterior descending artery
- absent left main trunk (split origination of LCA)
- coronary hypoplasia
- ectopic origin
- anomalous left coronary artery off the pulmonary artery (ALCAPA)
-
anomalous aortic origin of coronary artery
- origination of a coronary artery from the opposite sinus (ACAOS)
- single coronary artery
- LCA or RCA (or a branch of either artery) arising from the non-coronary sinus
- LCx and LAD arising separately from the left coronary sinus
- anomalous location of coronary ostia
- from sinotubular junction
- from ascending aorta
- split artery origins
- anomalous course of coronary arteries
- absent coronary artery
- anomalies of intrinsic coronary arterial anatomy
- congenital ostial stenosis or atresia (LCA, LAD, RCA, Cx)
- coronary ostial dimple
- coronary ectasia or aneurysm
- intramural coronary artery (myocardial bridging)
- subendocardial coronary course
- coronary crossing
- anomalous origin of posterior descending artery (PDA) from the anterior descending branch or a septal penetrating branch
- dual right coronary artery
- dual left anterior descending artery
-
anomalies in coronary arterial termination
- inadequate arteriolar/capillary ramifications
- presence of fistulation from terminal coronary arteries to various structures (coronary arteriovenous fistula)
- extracardiac termination
Related articles: Anatomy: Thoracic
- thoracic skeleton[+][+]
- thoracic cage
- thoracic spine
- articulations
- muscles of the thorax[+][+]
- diaphragm
- intercostal space
- intercostal muscles
- variant anatomy
- spaces of the thorax[+][+]
- thoracic viscera[+][+]
- lower respiratory tract
-
heart
- cardiac chambers
- heart valves
- cardiac fibrous skeleton
- innervation of the heart
- development of the heart
- cardiac wall
-
pericardium
- epicardium
- epicardial fat pad
- pericardial space
- oblique pericardial sinus
- transverse pericardial sinus
-
pericardial recesses
- aortic recesses
- pulmonic recesses
- postcaval recess
- pulmonary venous recesses
- pericardial ligaments
- myocardium
- endocardium
-
pericardium
- esophagus
- thymus
- breast
- arterial supply of the thorax
-
thoracic aorta (development)
-
ascending aorta
-
aortic root
- aortic annulus
-
coronary arteries
- coronary arterial dominance
- myocardial segments
-
left main coronary artery (LMCA)[+][+]
- ramus intermedius artery (RI)
-
circumflex artery (LCx)
- obtuse marginal branches (OM1, OM2, etc))
- Kugel's artery
-
left anterior descending artery (LAD)
- diagonal branches (D1, D2, etc)
- septal perforators (S1, S2, etc)
-
right coronary artery (RCA)[+][+]
- conus artery
- sinoatrial nodal artery
- acute marginal branches (AM1, AM2, etc)
- inferior interventricular artery (PDA)
- posterior left ventricular artery (PLV)
- congenital anomalies
- sinotubular junction
-
aortic root
- aortic arch[+][+]
- aortic isthmus[+][+]
- descending aorta[+][+]
-
ascending aorta
- pulmonary trunk[+][+]
-
thoracic aorta (development)
- venous drainage of the thorax[+][+]
- superior vena cava (SVC)
- inferior vena cava (IVC)
-
coronary veins
-
cardiac veins which drain into the coronary sinus
- great cardiac vein
- middle cardiac vein
- small cardiac vein
- posterior vein of the left ventricle
- vein of Marshall (oblique vein of the left atrium)
- anterior cardiac veins
- venae cordis minimae (smallest cardiac veins or thebesian veins)
-
cardiac veins which drain into the coronary sinus
- pulmonary veins
- bronchial veins
- thoracoepigastric vein
- lymphatics of the thorax[+][+]
- innervation of the thorax[+][+]










 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.