
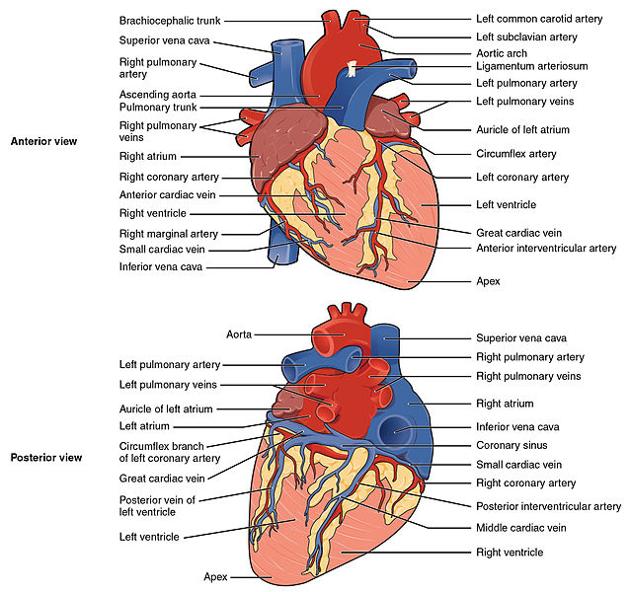
The right atrium (RA) (plural: atria) is one of the four chambers of the human heart and receives deoxygenated blood from the two venae cavae and the coronary sinus. Outflow is the through the tricuspid valve to the right ventricle (RV). The sino-atrial node (SA node) lies at the junction of the superior vena cava (SVC) and the right atrium and is the main pacemaker of the heart.
On this page:
Gross anatomy
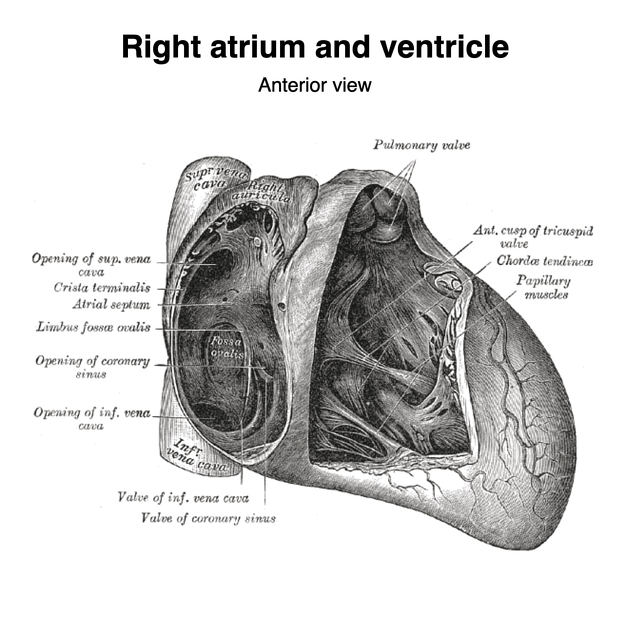
The right atrium receives deoxygenated blood from the superior vena cava (SVC), the inferior vena cava (IVC), the coronary sinus (covered by the Thebesian valve), and the Thebesian veins.
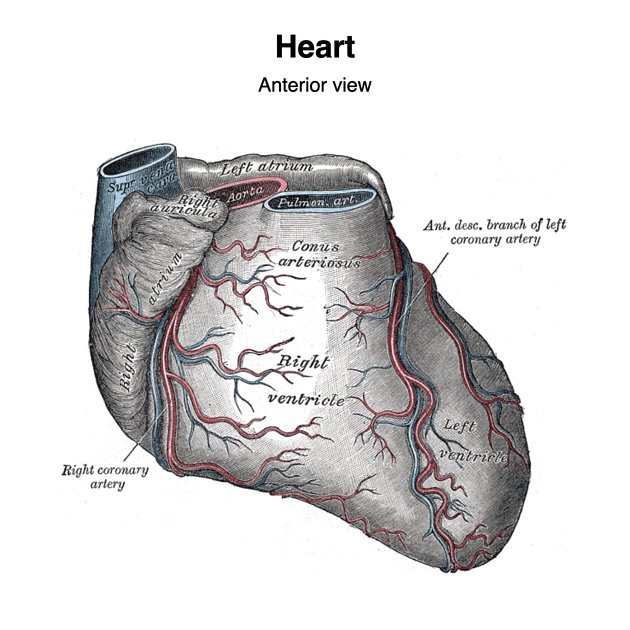
It is grossly the shape of an irregular ellipsoid, with the exception of the right atrial appendage (auricle), which arises anteriorly. The right atrial appendage overlies the aortic root and the proximal right coronary artery (RCA) 5.
The right atrium is separated from the left atrium by the interatrial septum. In cases of congenital cardiac malformations, the morphologic right atrium can be identified by the fossa ovalis in the interatrial septum 5.
The right atrium leads into the right ventricle through the tricuspid valve.
Boundaries
superior end: SVC orifice
inferior end: IVC orifice
posterior wall: interatrial septum, faces anterior and to the right, marked by depression (fossa ovalis) in lower part of the septum with crescenteric upper margin called the limbus)
anterior and right lateral wall: cardiac wall
left lateral extent: right atrioventricular ostium
Parts
-
atrial cavity divided into 2 main parts by crista terminalis
smooth muscular ridge (musculi pectini) from the roof just in front of and below the SVC opening (between SVC and right auricle) and extends along lateral wall to the anterior lip of IVC 5
-
sinus venarum cavarum
cavity posterior to crista terminalis
drains IVC and SVC
smooth wall
-
atrium proper
-
anterior half of the chamber (anterior to crista terminalis)
represents true auricular chamber of embryonic heart
-
includes right auricle
upper end of right atrium to the left of the SVC
overlaps commencement of aorta and clasps infundibulum of right ventricle
-
wall is ridged by pectinate muscles fanning out from crista terminalis and also extending into the right atrial appendage
the atrial lead of an external pacemaker is frequently located in these muscles
-
Openings
-
SVC opening superiorly
superiorly to the right of the crista
-
IVC opening inferiorly
guarded by ridge that extends from anterior lip of IVC (remains of valve of IVC / Eustachian valve)
-
coronary sinus opening inferiorly
medial to the IVC opening in posterior wall of right atrium
bordered by small fold (valve of coronary sinus / thebesian valve)
-
right atrioventricular ostium
guarded by tricuspid valve
Relations
superior: SVC
inferior: IVC
left lateral: right ventricle, aortic root and valve
right lateral: right lung and pleura, phrenic nerve, pericardiophrenic artery and vein
posterior: left atrium, right pulmonary veins
Arterial supply
-
primarily from the right coronary artery (RCA) and several of its branches:
conus artery (first branch off RCA in 55%, otherwise arises off left circumflex artery)
sinoatrial node artery (usually second branch off RCA in 60%)
Venous drainage
variable veins drain the atrial walls
tiny myocardial Thebesian veins drain directly into the right atrium
Innervation
-
primary cardiac pacemaker
subepicardial location near junction of SVC and right atrium
regulated by vagus nerve and cardiac sympathetic plexus
-
subendocardial location between coronary sinus ostium, septal leaflet of tricuspid valve and tendon of Todaro (which connects the Thebesian and eustachian valves), an area known as the Triangle of Koch
Variant anatomy
-
thickened Eustachian valve of the IVC
thickened ridge due to incomplete regression of Eustachian valve
a prominent pectinate muscle is present in most people known as the taenia sagittalis
incomplete closure of the foramen ovale
variable size of the fossa ovalis
coronary sinus may be doubled
coronary sinus may drain into the left atrium
SVC may be joined to the left atrium
Radiographic features
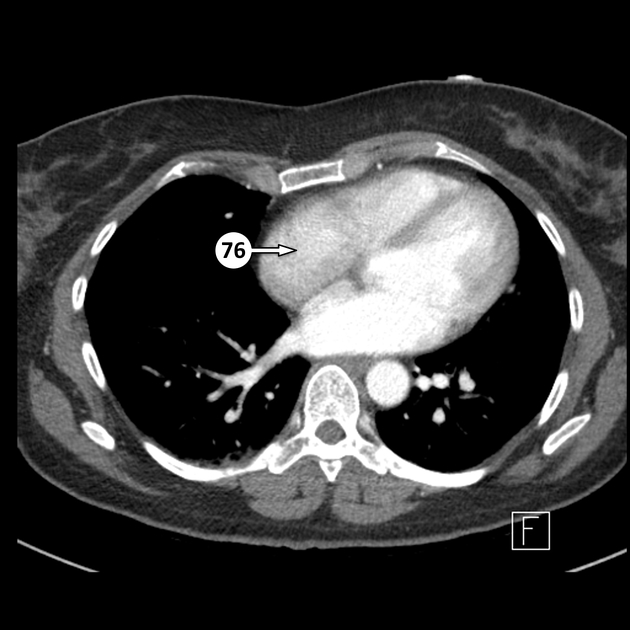
On contrast-enhanced chest CT and cardiac MRI, the right atrium when measured on axial slices can be considered enlarged when the transverse diameter is ≥67 mm (male) and ≥64 mm (female) 3.
Development
Develops from the right horn of the sinus venosus. Originates as two chambers, an anterior and a posterior. See development of the heart.
Practical points
CT evaluation of the right atrium:
the patient should be encouraged to avoid the Valsalva maneuver, which may bring unopacified blood from the IVC into the right atrium, and may mimic a thrombus
to avoid streak artifact from dense CT contrast, a multiphasic study with 100% contrast followed by a 20-50% contrast and saline chaser should be administered
Size
Ultrasound
Echocardiography
Measurements of the right atrium are primarily acquired from the transthoracic apical four chamber view. While more time intensive, planimetry is preferred to estimations of area based on long/short axis dimensions. Measurements are obtained as follows 4:
-
major dimension
measured parallel to the interatrial septum from the center of the tricuspid annulus to the superior atrial wall
-
minor dimension
perpendicular to the long axis, measured from the interatrial septum to the atrial free wall
-
end-systolic area
the atrial endocardium is traced, spanning the lateral to septal aspects of the tricuspid annulus
The lower and upper limits of reference values for the right atrium are as follows:
major dimension: 3.4-5.3 cm
minor dimension: 2.6-4.4 cm
end-systolic area: 10-18 cm2
History and etymology
"Atrium" is the Latin word for "court", referring to the central area in a Roman house from which one could enter various chambers. It was entered through the "ostium" of a Roman house.




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.