
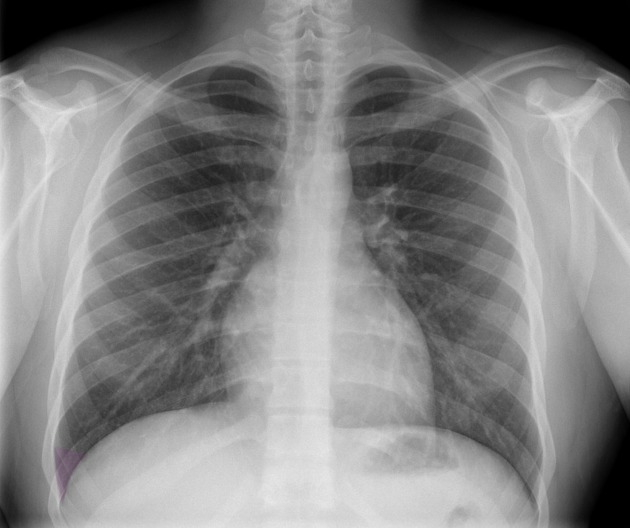
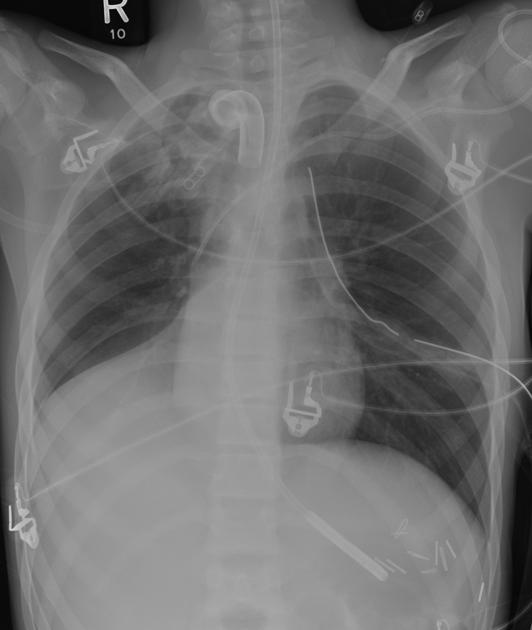
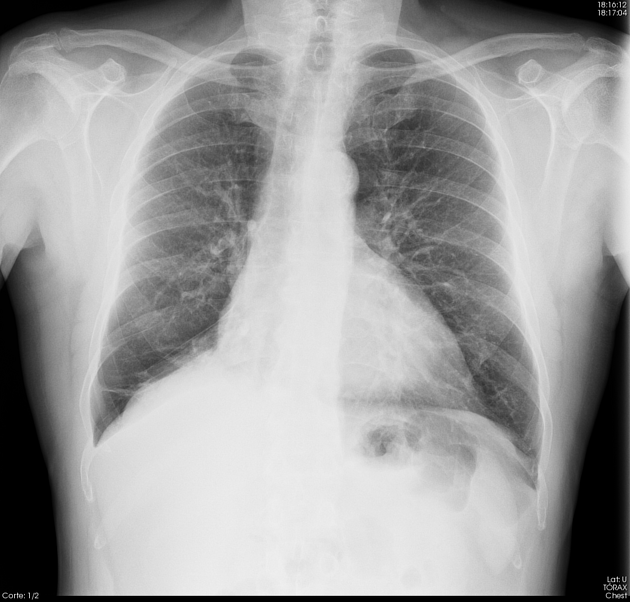
Right lower lobe (RLL) collapse forms a triangular opacity extending from the hilum to the diaphragm. There is less overlap with the heart shadow compared to left lower lobe collapse.
Findings of lower lobe collapse can be grouped together as they are almost identical on both sides.
For a general discussion please refer to the article on lobar collapse.
On this page:
Radiographic features
Plain radiograph
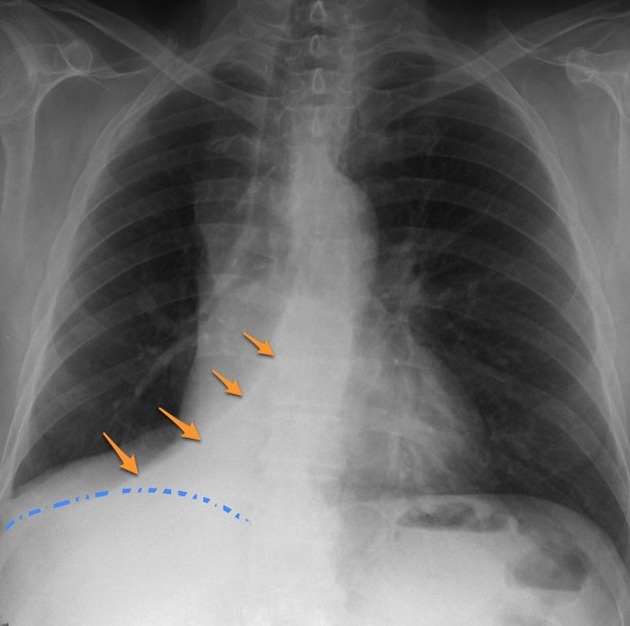
Collapse of the right lower lobe is usually easily identified but can be missed if collapse is profound (which may occur when consolidation is absent), or if the patient is rotated. Features include: 1-3:
triangular opacity in the right lower zone (usually medially) with the apex pointing towards the right hilum
obscured medial right hemidiaphragm
inferior displacement of the right hilum
obscured descending interlobar pulmonary artery
distinct right heart border in contact with normal middle lobe
inferior displacement of the horizontal fissure
Non-specific signs indicating right sided atelectasis may also be present.
They include:
elevation of the right hemidiaphragm
crowding of the right sided ribs
shift of the mediastinum to the right
ipselateral hypertransradiancy and wider spacing of blood vessels due to compensatory hyperinflation of the right upper and middle lobes
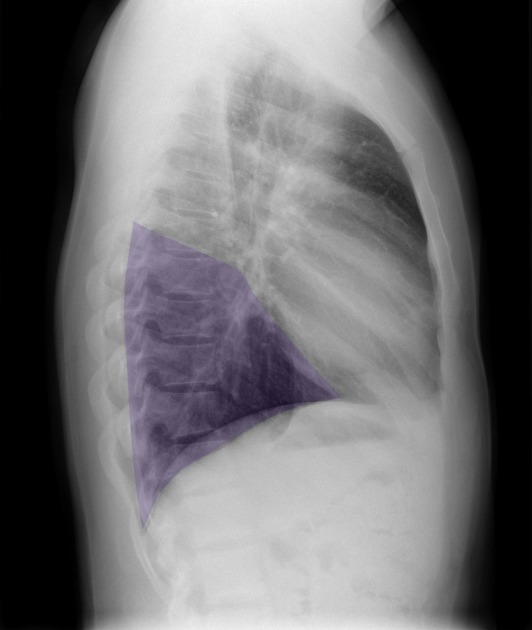
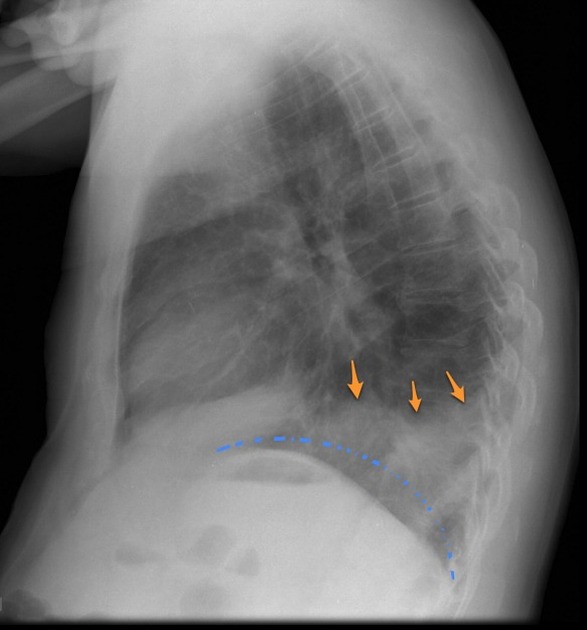
On the lateral projection the findings are usually obvious:
triangular opacity in the lower posterior chest
posterior right hemidiaphragm obscured
increased attenuation over the lower thoracic vertebrae, (reversing the normal pattern of decreased attenuation compared with the upper thoracic vertebrae) 3
oblique fissure displaced posteroinferiorly
invisible oblique fissure on lateral CXR if profound collapse rotates the fissure posteromedially (non-tangential to the x-ray beam) 2
inferior displacement of the right hilum
If there is an obstructing lesion in the bronchus intermedius, there will be signs of both RML and RLL collapse.
CT
triangular opacification in axial images, thinner at the hilum, against the posterior mediastinum/spine and medial hemidiaphragm 2
oblique fissure pulled posteriorly and may rotate posteromedially 2
compensatory hyperinflation of the right upper and middle lobes 2
Differential diagnosis
The features of right lower lobe collapse are distinctive, however consider:
combined right middle and lower lobe collapse if the heart border is obscured
consolidation of the medial basal segment of the right lower lobe
pulmonary or posterior mediastinal mass
This location is also common for pulmonary sequestration.





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.