
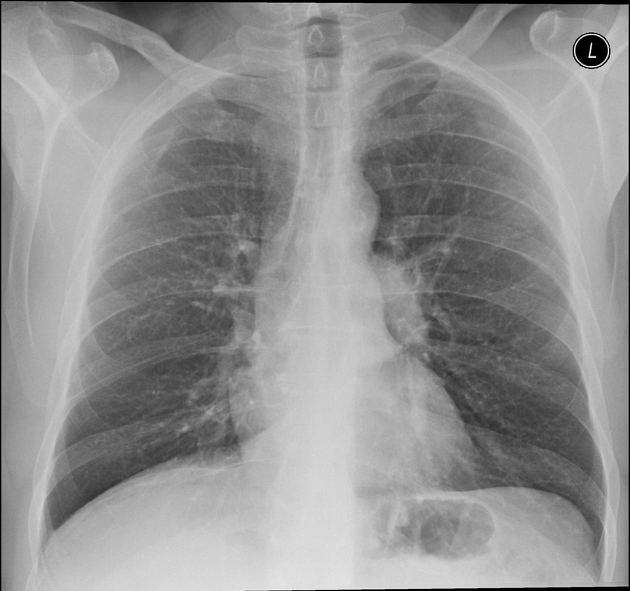
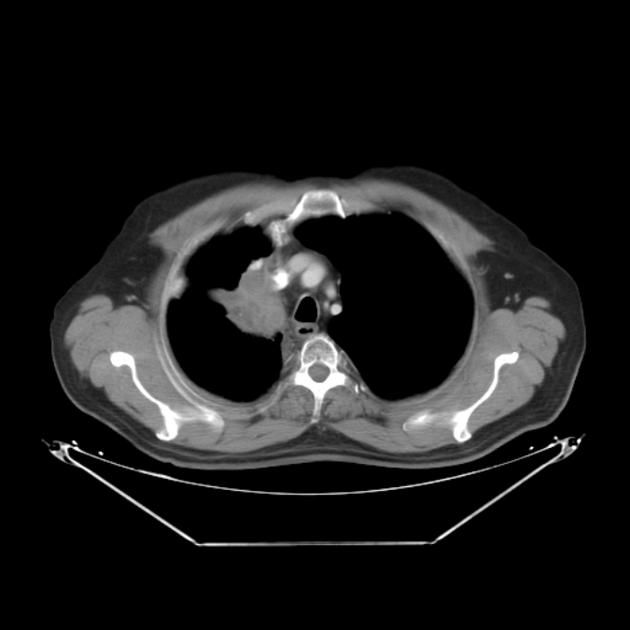
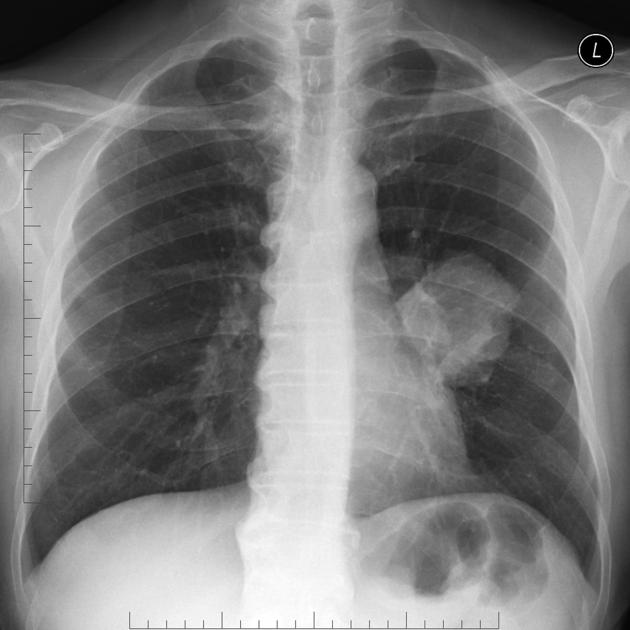
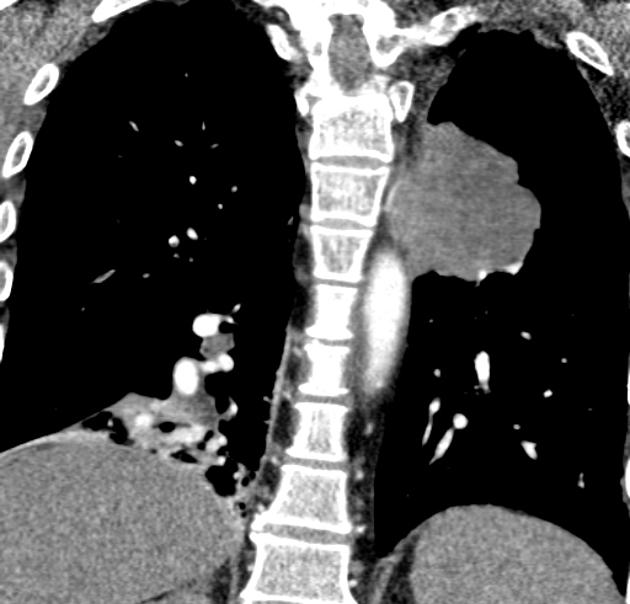
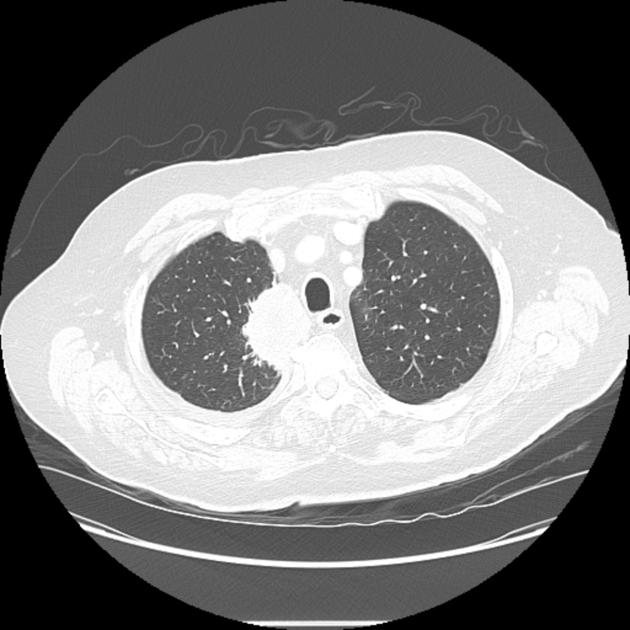
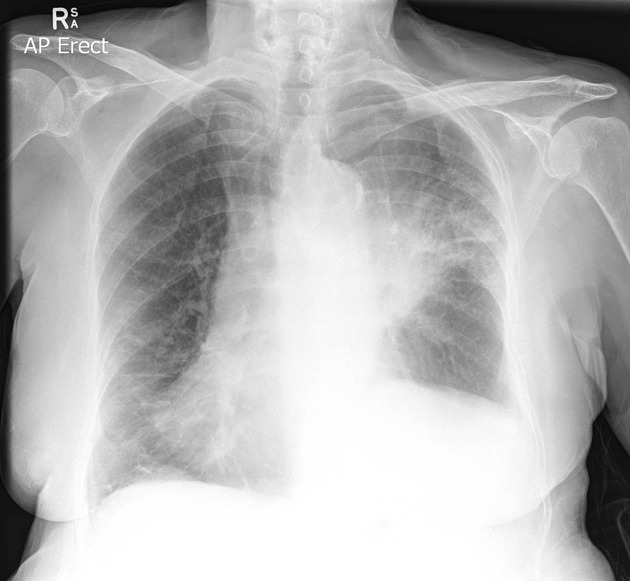
Primary lung cancer refers to uncontrolled growth of any component of the lung. In 2023 the WHO stated that lung cancer is the most common cause of cancer-related deaths in men and women globally and that 85% of lung cancer cases are related to smoking.
This article gives an overview of the histological subtypes focussing on their common aspects; for more information please refer to the articles on each subtype described below.
On this page:
Terminology
Bronchogenic carcinoma is a term that is frequently used as a synonym for lung cancer but is inaccurate because lung cancers can arise any lung component, not just the airways 17.
Epidemiology
Lung cancer is a leading type of cancer, roughly equal in prevalence to breast cancer 13. It is the leading cause of cancer mortality worldwide; accounting for ~20% of all cancer deaths 1.
Risk factors
The major risk factor is tobacco smoking, implicated in 85% of cases. This increases the risk of lung cancer depending on histological subtype 10:
squamous cell lung cancer: 11x (men), 15x (women)
small cell lung cancer: 10x (men), 25x (women)
large cell lung cancer: 7x (men), 8x (women)
lung adenocarcinoma: 4x (men and women)
Other risk factors:
asbestos: 5x increased risk
occupational exposure: uranium, radon, arsenic, chromium
diffuse lung fibrosis: 10x increased risk
air pollution
Associations
Various paraneoplastic syndromes can arise in the setting of lung cancer:
-
endocrine/metabolic
SIADH causing hyponatremia: small-cell subtype
ACTH secretion (Cushing syndrome): carcinoid and small-cell subtypes
adrenal insufficiency (Addison disease): from bilateral metastases 7
hyperparathyroidism: NSCLC can produce parathyroid hormone (extremely rare) 8
hypocalcemia: occurs in the setting of skeletal metastases; especially associated with NSCLC 6
PTH-related peptide (PTHrp) causing hypercalcemia: squamous cell carcinoma
-
neurological
polyneuropathy
myelopathy
limbic encephalitis: particularly associated with SCLC 9
-
other
hypertrophic pulmonary osteoarthropathy (HPOA): non-small cell 18
thrombophlebitis: adenocarcinoma subtype
Clinical presentation
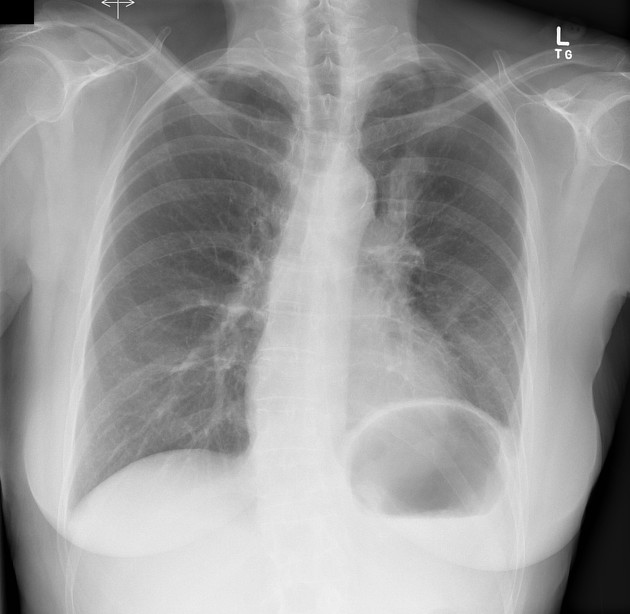
Patients with lung cancer may be asymptomatic in up to 50% of cases. Cough and dyspnea are rather non-specific symptoms that are common amongst those with lung cancer.
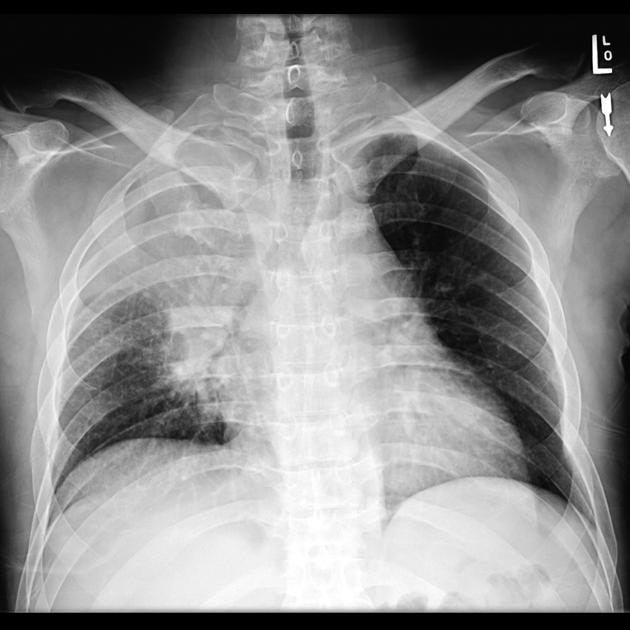
Central tumors may result in hemoptysis and peripheral lesions with pleuritic chest pain.
Pneumonia, pleural effusion, wheeze, lymphadenopathy are not uncommon. Other symptoms may be secondary to metastases (bone, contralateral lung, brain, adrenal glands, and liver, in frequency order for NSCLC 12) or paraneoplastic syndromes.
Pathology
The term bronchogenic carcinoma is somewhat loosely used to refer to primary malignancies of the lung that are associated with inhaled carcinogens 1 and includes four main histological subtypes. These are broadly divided into non-small cell carcinoma and small cell carcinoma as they differ clinically regarding presentation, treatment, and prognosis:
-
non-small cell lung cancer (NSCLC) (80%)
-
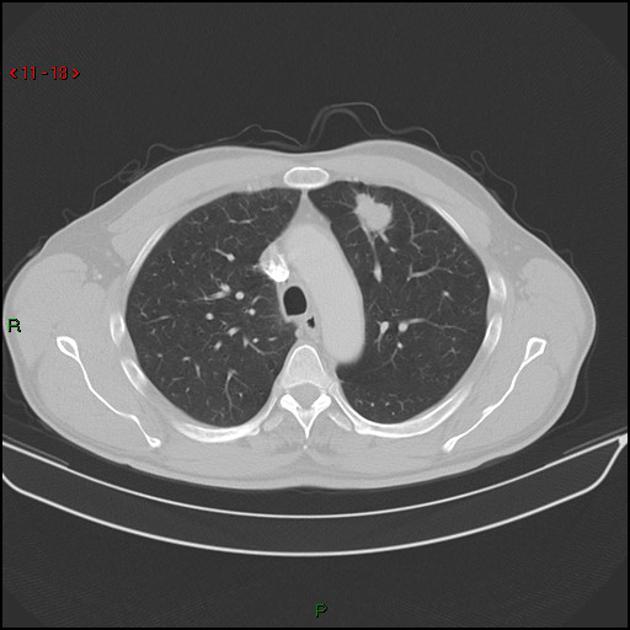
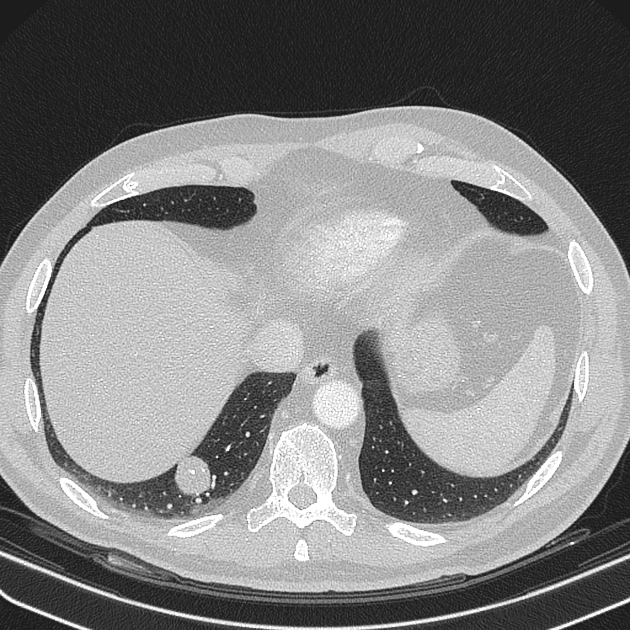
adenocarcinoma (35%)
most common cell type overall
most common in women
most common cell type in non-smokers but still most patients are smokers
peripheral
-
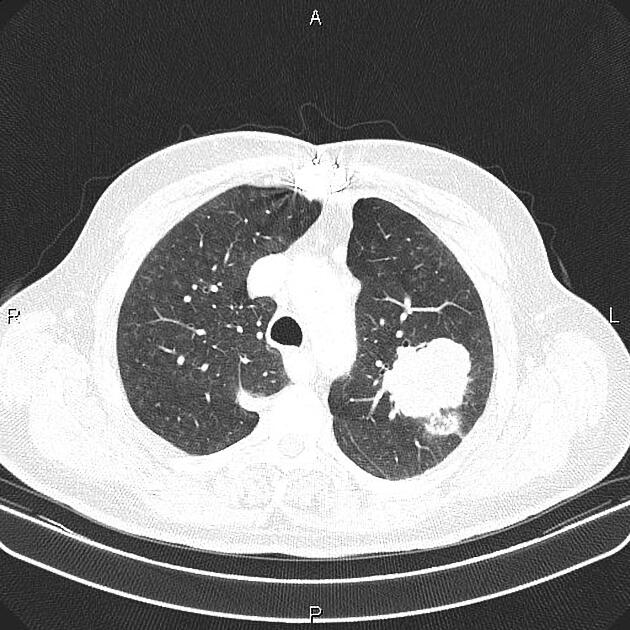
squamous cell carcinoma (30%)
strongly associated with smoking
most common carcinoma to cavitate
poor prognosis
-
large-cell carcinoma (15%)
peripherally located
very large, usually >4 cm
-
-
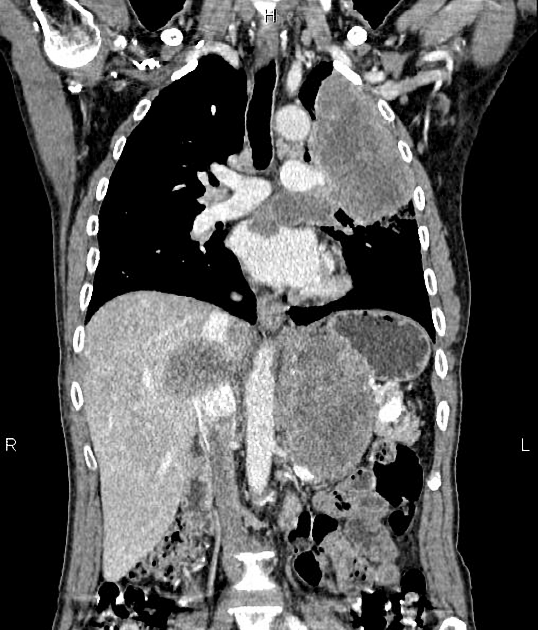
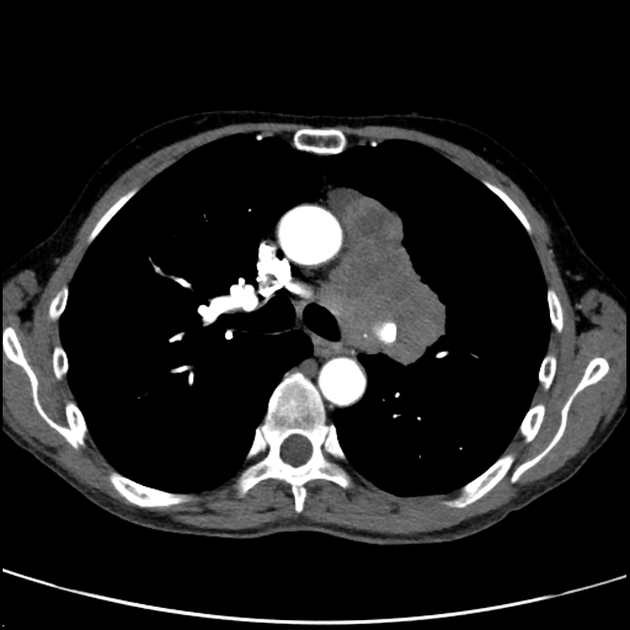
small cell lung cancer (SCLC) (20%)
almost always in smokers
metastasizes early
most common primary lung malignancy to cause paraneoplastic syndromes and SVC obstruction
worst prognosis
Other malignant pulmonary neoplasms include lymphoma and sarcoma (rare).
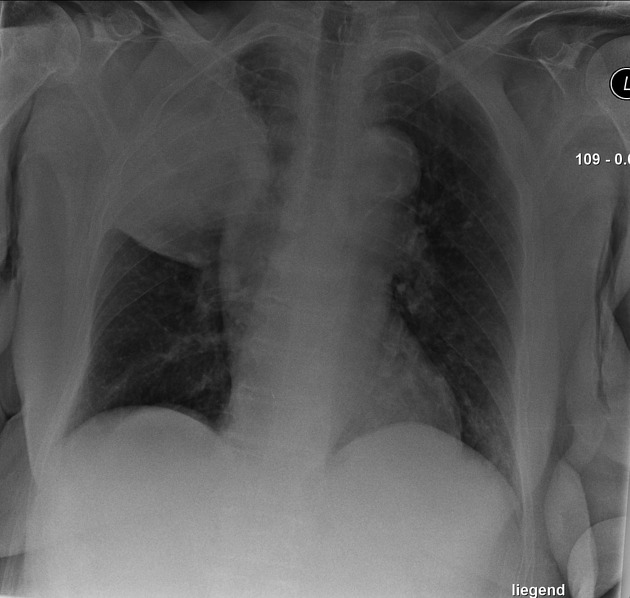
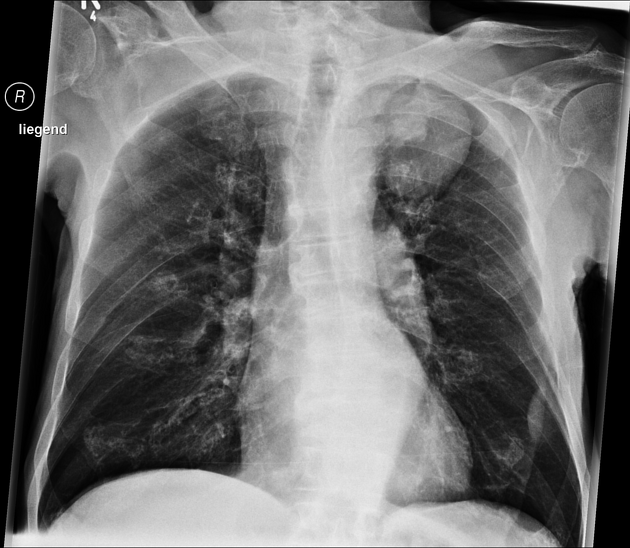
Each subtype has different radiographic appearances, demographics, and prognoses:
Markers
Several antibodies or markers from tissue samples may be useful in the diagnosis and prognostication of disease. These include
programmed death-ligand 1 (PD-L1)-targeted monoclonal antibodies
thyroid transcription factor 1 (TTF-1): expressed in most lung cancer except squamous cell cancer
Genetics
ROS1 mutation: 1-2% of NSCLC 15; more common in females 14
ALK mutation: 2-5% of NSCLC; more common in males, younger, light/never smokers, and more likely to be adenocarcinoma presenting with advanced disease 16 (see: main article)
Staging
according to the IASLC (International Association for the Study of Lung Cancer) 8th edition lung cancer staging system
previously small cell and non-small cell lung cancers were staged differently, but since 2013 all lung cancers are staged the same way
Treatment and prognosis
Treatment and prognosis vary not only with stage but also with cell type. In general, surgery, chemotherapy, and radiotherapy are offered according to the stage, resectability, operability, and functional status. Targeted treatments depend on molecular testing, e.g. ALK mutated lung cancers can be treated with ALK-inhibitors (e.g. crizotinib) 16.
Non-small cell carcinoma
-
treatment
operable disease (stage I to IIIA): surgery
unresectable disease: neoadjuvant chemotherapy, radiotherapy
advanced disease: palliative combined chemotherapy
-
prognosis (5-year survival rates):
local (stage I): 55-67%
locally advanced (stages II-IIIA): 23-40%
advanced (stages IIIB and IV): 1-3%
Small-cell carcinoma
-
treatment
limited disease: chemoradiotherapy
extensive disease: palliative combined chemotherapy
-
prognosis: poor
limited: 5-year survival rate 15-25%
extensive: 2-year survival 20% (with palliative combined chemotherapy and supportive care)
Differential diagnosis
venous collateral pathways - venous varices
















 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.