
Lung atelectasis (plural: atelectases) refers to lung collapse, which can be minor or profound and can be focal, lobar or multilobar depending on the cause.
On this page:
Terminology
According to the fourth Fleischner glossary of terms, atelectasis is synonymous with collapse 13.
Pathology
Atelectasis is a radiopathological sign that can be categorized in many ways. Each approach aims to help identify possible underlying causes together with other accompanying radiological and clinical findings.
Atelectasis can be subcategorised based on the underlying mechanism, as follows:
-
resorptive (obstructive) atelectasis
occurs as a result of complete obstruction of an airway
no new air can enter the portion of the lung distal to the obstruction, and any air that is already there is eventually absorbed into the pulmonary capillary system, leaving a collapsed section of the affected lung
because the visceral and parietal pleura do not separate in resorptive atelectasis, traction is created, and if the loss of volume is considerable, mobile thoracic structures may be pulled toward the side of volume loss ("mediastinal shift")
potential causes of resorptive atelectasis include obstructing neoplasms, mucus plugging in asthmatics or critically ill patients and foreign body aspiration
resorptive atelectasis of an entire lung ("collapsed lung") can result from complete obstruction of the right or left main bronchus
-
passive (relaxation) atelectasis
occurs when contact between the parietal and visceral pleura is disrupted with loss of normal negative pressure and the lung relaxes due to natural elastic recoil
the three most common specific etiologies of passive atelectasis are pleural effusion, pneumothorax and diaphragmatic abnormality
-
occurs as a result of any thoracic space-occupying lesion (e.g. large pneumothorax) compressing the lung and forcing air out of the alveoli
-
occurs as a result of scarring or fibrosis that reduces lung expansion
common etiologies include granulomatous disease, necrotizing pneumonia and radiation fibrosis
-
occurs from surfactant deficiency 2
depending on etiology, this deficiency may either be diffuse throughout the lungs or localized
-
gravity dependant atelectasis (dependent atelectasis)
in the most dependent portions of the lungs due to the weight of the lungs
osteophyte-induced adjacent pulmonary atelectasis and fibrosis
Atelectasis can also be subcategorised by morphology:
linear (a.k.a. plate, band, discoid) atelectasis: a minimal degree of collapse as seen in patients who are not taking deep breaths ("splinting"), such as postoperative patients or patients with rib fracture or pleuritic chest pain; this is very common
round atelectasis: classically associated with asbestos exposure
Lastly atelectasis can be described according to anatomical extent:
lung atelectasis: complete collapse of one lung
lobar atelectasis: collapse of one or more lobes of a lung.
segmental atelectasis: collapse of one or more individual pulmonary segments
subsegmental atelectasis: collapse of a portion of a pulmonary segment
Radiographic features
Vary depending on the underlying mechanism and type of atelectasis
Plain radiograph / CT
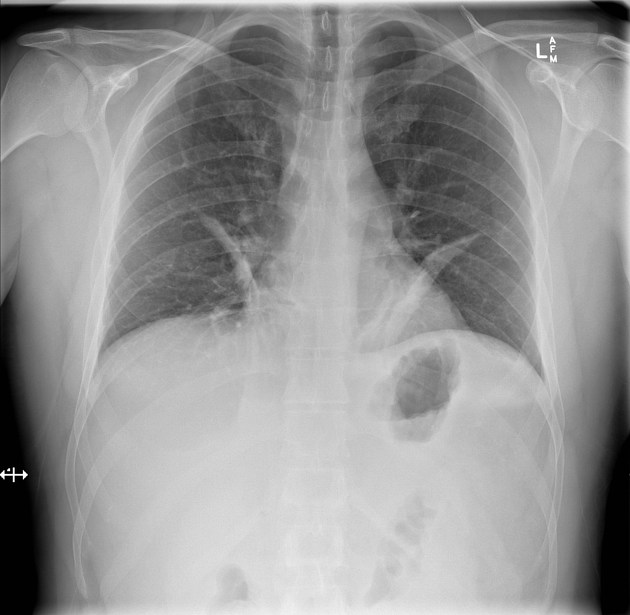
Direct signs of atelectasis
displacement of interlobar fissures
crowding together of pulmonary vessels
crowded air bronchograms (does not apply to all types of atelectasis; can be seen in subsegmental atelectasis due to small peripheral bronchi obstruction, usually by secretions; if the cause of the atelectasis is central bronchial obstruction, there will usually be no air bronchograms)
Indirect signs of atelectasis
pulmonary opacification
shifting granuloma (or any other previously documented lesion, used as a reference for comparison)
compensatory hyperexpansion of the surrounding or contralateral lung
displacement of the heart, mediastinum, trachea, hilum
propinquity of the ribs
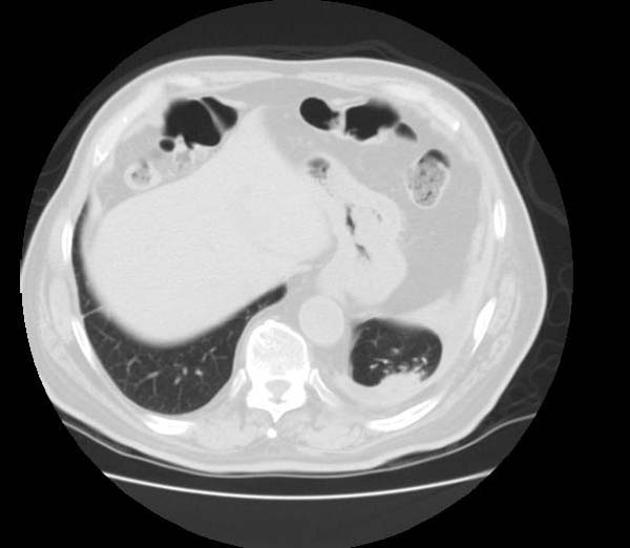
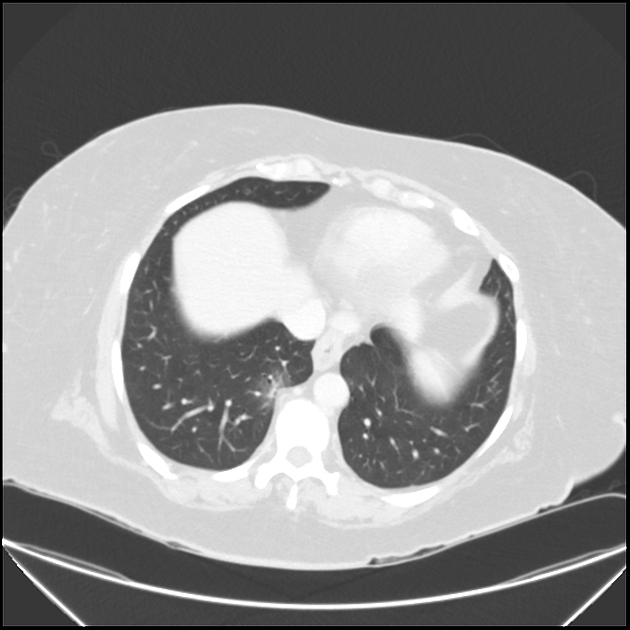
Resorptive (obstructive) atelectasis
increased density (opacity) of the atelectatic portion of lung
displacement of the fissures toward the area of atelectasis
upward displacement of hemidiaphragm ipsilateral to the side of atelectasis
crowding of pulmonary vessels and bronchi in region of atelectasis
+/- compensatory overinflation of unaffected lung
+/- displacement of thoracic structures (if atelectasis is substantial)
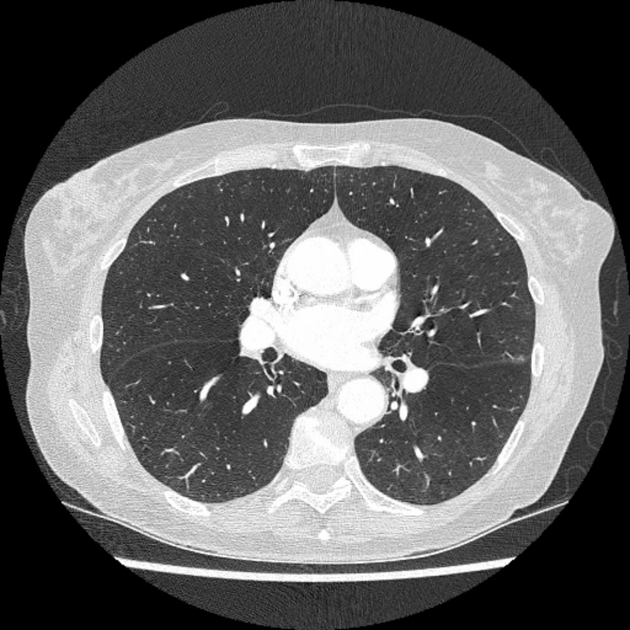
Linear (plate, discoid, subsegmental) atelectasis
relatively thin, linear densities in the lung bases oriented parallel to the diaphragm (known as Fleischner lines)
Ultrasound
The sonographic morphology of atelectatic lung may resemble hepatic parenchyma, often referred to as "tissue-like" or "hepatized" in appearance. Distinguishing features of atelectasis by etiology may appear as follows:
-
compressive atelectasis is most often visualized in the costophrenic recess bordered by a disproportionately large pleural effusion
low-level, homogenous echogenicity with few to no air bronchograms
margins are usually regular with a triangular shape 10
a shred sign may be present at the transition to aerated lung
-
obstructive atelectasis
early static air bronchograms due to distal air trapping
as the air is resorbed, bronchi may fill with fluid resulting in anechoic, tubular structures known as fluid bronchograms 11
may be differentiated from blood vessels with color flow Doppler
CT
Air bronchograms indicate patency of the proximal airways and the airways will be crowded indicating volume loss. If air bronchograms are absent suspect an obstructing lesion or mucoid impaction. In this latter case, bronchoscopy may be helpful.
Following IV contrast medium, atelectatic lung enhances more than skeletal muscle 12.
These features of volume loss and marked enhancement together with the absence of fever help to distinguish atelectasis from pneumonic consolidation.
History and etymology
Atelectasis comes from the Greek words 'ateles' and 'ektasis' translating to 'incomplete expansion' 6.





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.