
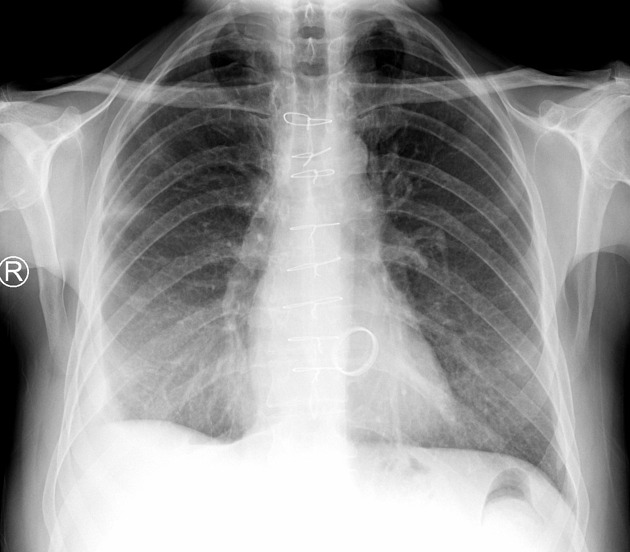
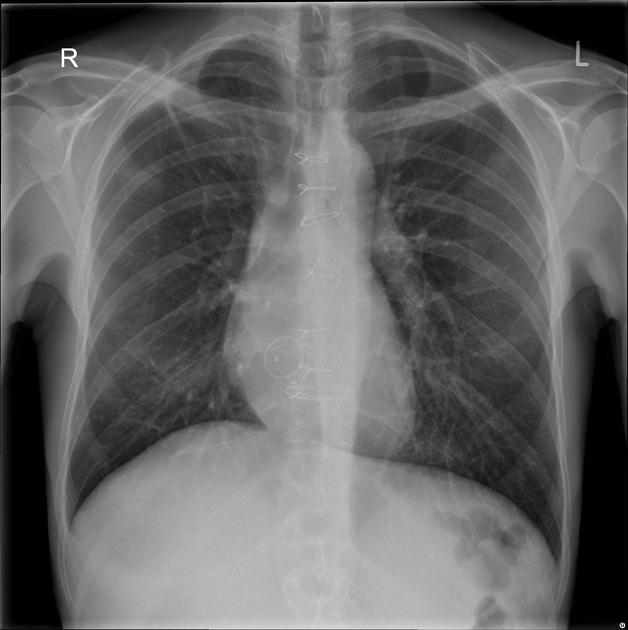
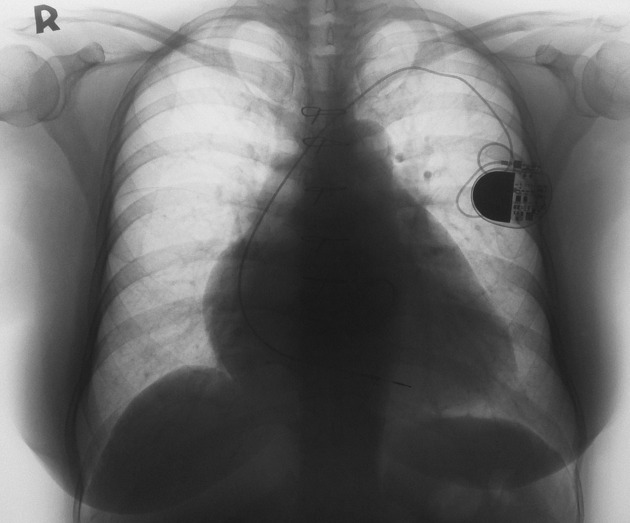
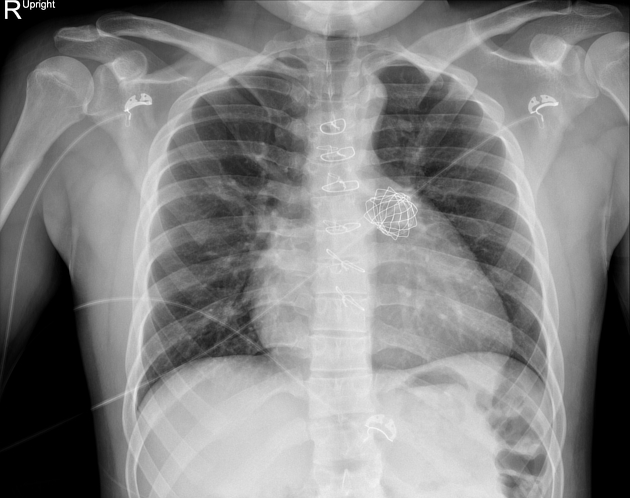
Prosthetic heart valves are common. The four valves of the heart may all be surgically replaced. However, the aortic and mitral valves are the most commonly replaced.
Replacements may be tissue or metallic valves, only the latter being visualized on imaging investigations. Sometimes the annulus alone is replaced as seen in annuloplasty rings.
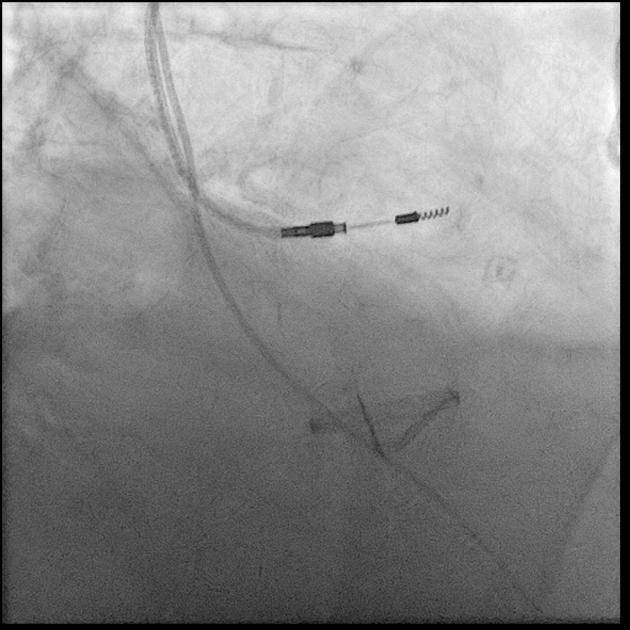
Aortic valves, in select circumstances, are being replaced via a transcatheter approach, called transcatheter aortic valve implantation (TAVI) from a femoral artery approach.
Radiographic features
Evaluation of prosthetic valves often relies on multimodality imaging, including transesophageal echocardiography, transthoracic echocardiography, fluoroscopy, and computed tomography (CT) 3.
Echocardiography
Valve appearance on echocardiography is dependent on the type of valve, which is generally subdivided into two categories (mechanical and bioprosthetic) with examples as follows 4,5:
-
mechanical valves
-
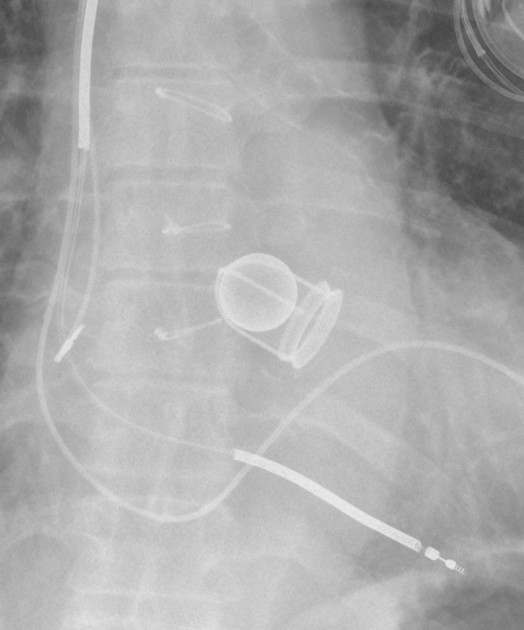
ball cage valves
Starr-Edwards caged ball valve
-
tilting disk valves
Bjork-Shiley tilting disk valve
-
-
bioprosthetic valves
homografts
heterografts
-
stented
Carpentier-Edwards stented aortic valve
-
stentless
Biocor stentless aortic valve
Transesophageal echocardiography is the modality of choice to assess the status of a prosthetic heart valve; a baseline study is typically performed after placement, and subsequent studies rely on comparison with this baseline to assess for pathology.
Complications of prosthetic valves
Complications include 5:
-
obstruction
-
maybe due to thrombus or pannus 4
-
differentiation on MDCT:
pannus appears as a circular or semicircular mass extending from the prosthesis ring, can demonstrate enhancement and typically shows a significantly higher attenuation as measured by Hounsfield units (HU) with a recommended cut-off point of >145 HU (sensitivity 88%, specificity 96%)
thrombus appears as an irregular lobulated non-enhancing mass
-
thrombogenic obstruction typically occurs with a subtherapeutic INR early after mechanical prosthesis implantation 6
typically occult to transthoracic echo studies
the posterior acoustic shadowing from the valve obscures the typical atrial location of thrombi
obstruction due to pannus tends to be a more chronic process, with slow symptom onset and in older valvular prosthesis
-
-
-
with or without valvular vegetation or paravalvular abscess
paravalvular regurgitation
-
valve failure (see below)
mechanical failure in mechanical valves
degeneration of a biological valve
hemolytic anemia: rare, both biological and mechanical valves 7
Severe dysfunction of a prosthetic valve should be suspected when the following parameters are measured 5:
-
-
severe regurgitation
vena contracta (VC) >0.6 cm
dense, triangular continuous wave Doppler envelope with an early peak
systolic flow reversal on pulmonary venous Doppler
-
severe stenosis
mitral inflow velocity peak >2.5 m/s
pressure half time >200 ms
-
-
-
severe stenosis
peak outflow velocity >4 m/s
a ratio of the aortic velocity time integral (VTI) to the left ventricular outflow tract (LVOT) VTI less than 0.25
-
severe regurgitation
Doppler studies of the descending aorta show holodiastolic flow reversal
regurgitant jet fills more than 65% of the LVOT
-







 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.