
Complete hydatidiform mole
Citation, DOI, disclosures and article data
At the time the article was created The Radswiki had no recorded disclosures.
View The Radswiki's current disclosuresAt the time the article was last revised Henry Knipe had the following disclosures:
- Micro-X Ltd, Shareholder (past)
These were assessed during peer review and were determined to not be relevant to the changes that were made.
View Henry Knipe's current disclosures- Complete mole
- Complete molar pregnancy
- Complete hydatidiform mole (CHM)
- Classic hydatidiform mole
- Classic hydatidiform moles
- Complete hydatidiform moles (CHMs)
- Complete moles
- Complete molar pregnancies
Complete hydatidiform moles (CHM) are a type of molar pregnancy and fall at the benign end of the spectrum of gestational trophoblastic disease.
On this page:
Epidemiology
A complete hydatidiform mole is the most common type of gestational trophoblastic disease.
Pathology
Complete moles are characterized by the absence of a fetus or fetal parts (i.e. no embryonic tissues). There is a non-invasive, diffuse swelling of chorionic villi.
Significant difference is seen among the pathologists in the diagnosis of molar pregnancies just based on histopathological examination of the products of conception (POC) 8. The p57KIP2 gene is paternally imprinted and expressed from the maternal allele 8,9. Polymer-based immunohistochemistry (IHC) with p57, shows absent staining in the complete mole (CM) and positive staining in the hydropic abortus (HA) and partial mole (PM) 8,9. This IHC staining is a useful and inexpensive tool that can help distinguish a complete mole from its mimics and avoid DNA analysis 8,9.
Genetics
Approximately 90% of complete hydatidiform moles have a 46XX diploid chromosomal pattern, with ~10% having a 46XY composition. All the chromosomes are derived from the sperm, suggesting fertilisation of a single egg that has lost its chromosomes.
Markers
Serum beta HCG levels are markedly elevated, out of proportion to the pregnancy.
Radiographic features
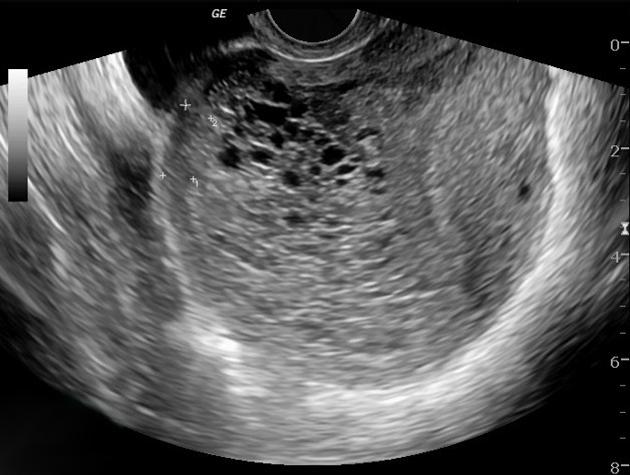
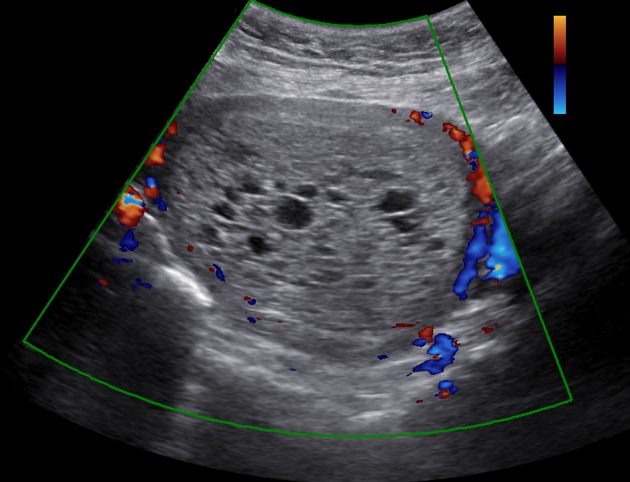
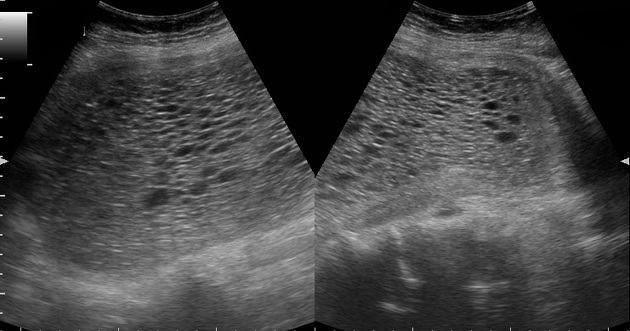
Ultrasound
enlarged uterus
-
may be seen as an intrauterine mass with cystic spaces without any associated fetal parts
the multiple cystic structures classically give a "snowstorm" or "bunch of grapes" type appearance.
-
may be difficult to diagnose in the first trimester 6
may appear similar to a normal pregnancy or as an empty gestational sac
<50% are diagnosed in the first trimester
bilateral theca lutein cysts may also be seen on ultrasound
color Doppler interrogation may show high velocity with a low impedance flow
CT
CT evaluation is not usually performed due to its low resolution for the uterine assessment. CT may show an enlarged uterus with areas of low attenuation, or hypoattenuating foci surrounded by highly enhanced areas in the myometrium.
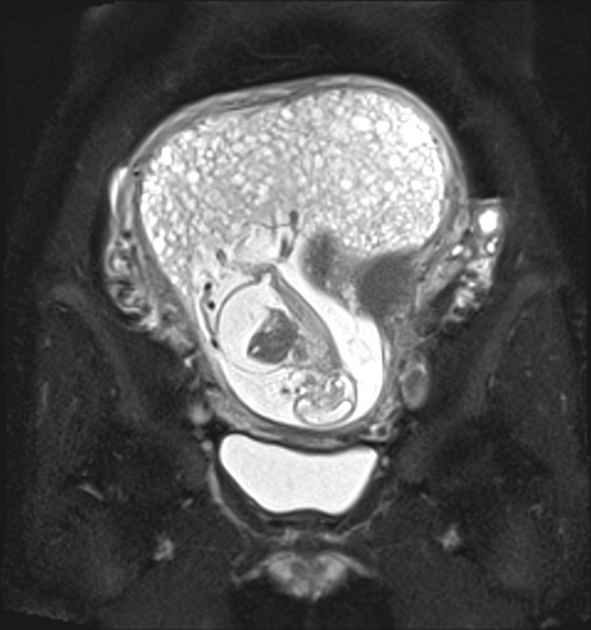
MRI
MRI may demonstrate a heterogeneous mass with cystic spaces distending the uterine cavity. Fetal parts are notably absent. Uterine zonal anatomy is often distorted although a hypointense irregular myometrial boundary may be seen 3. MRI may also demonstrate bilateral theca lutein cysts ref.
Signal characteristics
T1: may be areas of high signal corresponding to foci of hemorrhage
T2: heterogeneous high signal from the cystic spaces
T1 C+ (Gd): often intense enhancement due to hypervascularity
Treatment and prognosis
Suction and curettage are used for evacuation and are usually the routine treatment. Serial beta hCG levels are performed until it is no longer detectable on the assay, as it is the main indicator of residual disease.
A complete mole is itself benign but is considered a premalignant lesion. Degeneration into more invasive and malignant types of gestational trophoblastic disease can occur in ~15% (range 10-20%) of cases ref.
See also
References
- 1. Reuter K, Michlewitz H, Kahn P. Early Appearance of Hydatidiform Mole by Ultrasound. AJR Am J Roentgenol. 1980;134(3):588-9. doi:10.2214/ajr.134.3.588 - Pubmed
- 2. E. Albert Reece, Robert L. Barbieri. Obstetrics and Gynecology. (2010) ISBN: 9783131439512 - Google Books
- 3. Richard C. Semelka. Abdominal-Pelvic MRI, 2 Volume Set. (2010) - Google Books
- 4. Fowler D, Lindsay I, Seckl M, Sebire N. Routine Pre-Evacuation Ultrasound Diagnosis of Hydatidiform Mole: Experience of More Than 1000 Cases from a Regional Referral Center. Ultrasound Obstet Gynecol. 2006;27(1):56-60. doi:10.1002/uog.2592 - Pubmed
- 5. Benson C, Genest D, Bernstein M, Soto-Wright V, Goldstein D, Berkowitz R. Sonographic Appearance of First Trimester Complete Hydatidiform Moles. Ultrasound Obstet Gynecol. 2000;16(2):188-91. doi:10.1046/j.1469-0705.2000.00201.x - Pubmed
- 6. Lazarus E, Hulka C, Siewert B, Levine D. Sonographic Appearance of Early Complete Molar Pregnancies. J Ultrasound Med. 1999;18(9):589-94; quiz 595. doi:10.7863/jum.1999.18.9.589 - Pubmed
- 7. Marisa R. Nucci, MD, Esther Oliva, MD. Gynecologic Pathology. (2009) ISBN: 9780443069208 - Google Books
- 8. Kar R & Samadder A. Utility of P57 Immunohistochemistry in Differentiating Between Complete Mole, Partial Mole & Non-Molar or Hydropic Abortus. Indian J Med Res. 2017;145(1):133. doi:10.4103/ijmr.ijmr_982_15
- 9. Sasaki S, Sasaki Y, Kunimura T, Sekizawa A, Kojima Y, Iino K. Clinical Usefulness of Immunohistochemical Staining of P57 Kip2 for the Differential Diagnosis of Complete Mole. Biomed Res Int. 2015;2015:905648. doi:10.1155/2015/905648 - Pubmed
Incoming Links
- Gestational trophoblastic disease - complete hydatidiform mole
- Complete hydatidiform mole with bilateral theca leutin cysts
- Complete hydatidiform mole
- Complete hydatidiform mole
- Complete hydatidiform molar pregnancy
- Hydatidiform mole
- Complete hydatidiform molar pregnancy
- Partial hydatidiform mole
- Complete hydatidiform mole
- Complete hydatidiform mole
- Complete molar pregnancy and coexisting live fetus
- Complete hydatidiform mole
- Complete hydatidiform mole with bilateral theca lutein cysts
- Complete hydatidiform mole with bilateral theca lutein cysts
- Complete hydatidiform mole
Related articles: Pathology: Genitourinary
- obstetrics
-
first trimester
- ultrasound findings in early pregnancy
- embryo/fetus
- beta-hCG levels
- confirming intrauterine gestation
- pregnancy of unknown location (PUL)
- first trimester vaginal bleeding
- early structural scan
- aneuploidy testing
-
second trimester
- fetal biometry
- amniotic fluid volume
- fetal morphology assessment
- soft markers
- amnioreduction
- Doppler ultrasound
- nuchal translucency
- 11-13 weeks antenatal scan
- chorionic villus sampling (CVS) and amniocentesis
- other
- placenta
- placental anatomy
- placental developmental abnormalities
- placenta previa
- spectrum of abnormal placental villous adherence
- abnormalities of cord insertion
- abruptio placentae
- placental pathology
- vascular pathologies of placenta
- placental infections
- placental masses
- molar pregnancy
- twin placenta
- miscellaneous
-
first trimester
- gynecology
- acute pelvic pain
- chronic pelvic pain
- uterus
- ovaries
- ovarian follicle
- ovarian torsion
- pelvic inflammatory disease
- ovarian cysts and masses
- paraovarian cyst
- polycystic ovaries
- ovarian hyperstimulation syndrome
- post-hysterectomy ovary
- cervix
- fallopian tube
- other
- male genital tract
- prostate gland
- transrectal ultrasound
- prostate tumors
- infections of the prostate
-
prostatitis
- acute bacterial prostatitis
-
chronic prostatitis
- chronic bacterial prostatitis
- chronic prostatitis and chronic pelvic pain syndrome (CPPS)
- asymptomatic inflammatory prostatitis
- granulomatous prostatitis
- emphysematous prostatitis
- prostatic abscess
-
prostatitis
- benign prostatic hypertrophy
- cystic lesions of the prostate
- prostatic calcification
- prostatic infarction
- testes
-
unilateral testicular lesion
- testicular torsion
- orchitis
- testicular trauma
-
germ cell tumors of the testis
- testicular seminoma
-
non seminomatous germ cell tumors
- mixed germ cell tumor
- yolk sac tumor (endodermal sinus tumor)
- embryonal cell carcinoma
- choriocarcinoma
- testicular teratoma
- testicular epidermoid (teratoma with ectodermal elements only)
- burned out testis tumor
- sex cord / stromal tumors of the testis
- testicular cyst
- testicular lymphoma
- bilateral testicular lesion
- paratesticular lesions
- epididymis
- other
- polyorchidism
- cryptorchidism
- tubular ectasia of the rete testis
- cystadenoma of the rete testis
- testicular sarcoidosis
- testicular tuberculosis
- spermatic cord
- fibrous pseudotumor of the scrotum
- scrotal leiomyosarcoma
- testicular adrenal rest tumors (TARTs)
- tunica vaginalis testis mesothelioma
- splenogonadal fusion
- testicular vasculitis
- abnormal testicular Doppler flow (differential)
-
unilateral testicular lesion
- penis
- prostate gland
- KUB
- kidneys
- normal renal anatomy
- hydronephrosis
- urolithiasis
- renal masses
- renal cystic disease
- renal infection
- vascular
- trauma
- ureter
- normal ureter anatomy
- ureteral stricture
- ureteral dilatation
- ureteral anomalies
- ureteral tumors
- ureteral trauma
- other
- bladder
- kidneys
Related articles: Inspired signs
-
inanimate object inspired[+][+]
- accordion sign
- astronomical inspired
- ball of wool sign
- ball on tee sign (renal papillary necrosis)
- boot-shaped heart
- bowler hat sign
- bow tie sign
- box-shaped heart
- bucket handle appearance (disambiguation)
- chain of lakes sign
- champagne glass pelvis
- cobblestone appearance
- Coca-Cola bottle sign
- cockade sign (disambiguation)
- coin lesion
- collar button ulcer
- comb sign
- corduroy artifact
- corduroy sign
-
corkscrew sign (disambiguation)
- corkscrew sign (diffuse esophageal spasm)
- corkscrew sign (inner ear)
- corkscrew sign (midgut volvulus)
- crazy paving sign
- cupola sign
- curtain sign (lung ultrasound)
- dinner fork deformity
- dripping candle wax sign
- finger in glove sign
- fishhook ureters
- flame-shaped breast (gynecomastia)
- football sign (pneumoperitoneum)
- frozen pelvis
- ghost triad (gallbladder)
- ghost vertebra
- goblet sign
- ground glass opacity
- hockey stick sign (disambiguation)
- horseshoe (disambiguation)
- hourglass sign
- hurricane sign (cardiac SPECT)
- jail bar sign
- keyhole sign (disambiguation)
- leather bottle stomach
- light bulb sign (disambiguation)
- Lincoln log vertebra
- Mercedes-Benz sign (disambiguation)
- misty mesentery sign
- mosaic appearance (disambiguation)
- napkin ring sign
- open book fracture
- pearl necklace sign
- pencil in a cup
- picture frame vertebral body
- polka-dot sign
- rachitic rosary
- ribbon rib deformity
- ring shadow
- rugger jersey spine
- sack of marbles sign
- sail sign (disambiguation)
- scalpel sign
- spilled teacup sign
- stepladder sign (disambiguation)
-
string of pearls sign (disambiguation)
- string of pearls sign (abdominal radiograph of small bowel)
- string of pearls sign (polycystic ovarian syndrome)
- string of pearls sign (fibromuscular dysplasia)
- string of pearls sign (watershed infarction)
- Tam o' Shanter sign
- telephone receiver deformity
- thimble bladder
- tombstone iliac wings
- Venetian blind sign
- Venus necklace sign
- water bottle sign
-
weapon and munition inspired signs
- arrowhead sign
- bayonet artifact
- bayonet deformity
- boomerang sign (disambiguation)
- bullet-shaped vertebra
- cannonball metastases
- Cupid bow contour
- dagger sign
- double barrel sign
- halberd pelvis
- hatchet sign
- panzerherz
- pistol grip deformity
- saber-sheath trachea
- scimitar syndrome
-
target sign (disambiguation)
- double target sign (hepatic abscess)
- eccentric target sign (cerebral toxoplasmosis)
- reverse target sign (cirrhotic nodules)
- target sign (cholangiocarcinoma)
- target sign (choledocholithiasis)
- target sign (hepatic metastases)
- target sign (intussusception)
- target sign (neurofibromas)
- target sign (pyloric stenosis)
- target sign (tuberculosis)
- trident appearance
- Viking helmet sign
- white pyramid sign
- windswept knees
- wine bottle sign
-
vegetable and plant inspired[+][+]
- aubergine sign
- bamboo spine
- blade of grass sign
- celery stalk appearance (disambiguation)
- coconut left atrium
- coffee bean sign
- cotton wool appearance
- drooping lily sign
- ginkgo leaf sign (disambiguation)
- holly leaf sign
- iris sign
- ivy sign
- miliary opacities
- mistletoe sign
- onion signs (disambiguation)
- pine cone bladder
-
popcorn calcification (disambiguation)
- popcorn calcification (breast)
- popcorn calcification (chondroid lesions)
- popcorn calcification (fibrous dysplasia)
- popcorn calcification (osteogenesis imperfecta)
- popcorn calcification (pulmonary hamartomas)
- popcorn calcification (uterine fibroid)
- potato nodes
- rice signs (disambiguation)
- salt and pepper sign (disambiguation)
- tombstone iliac wings
- tree-in-bud
- tulip sign
- water lily sign
-
fruit inspired[+][+]
- apple core sign (disambiguation)
- apple-peel intestinal atresia
- banana and egg sign
- banana fracture
- banana sign
- berry aneurysm
- bowl of grapes sign
-
bunch of grapes sign (disambiguation)
- bunch of grapes sign (hydatidiform mole)
- bunch of grapes sign (bronchiectasis)
- bunch of grapes sign (IPMN)
- bunch of grapes sign (botryoid rhabdomyosarcoma)
- bunch of grapes sign (intracranial tuberculoma)
- bunch of grapes sign (intraosseous hemangiomas)
- bunch of grapes sign (multicystic dysplastic kidney)
- cashew nut sign
- lemon sign
- pear-shaped bladder
- strawberry gallbladder
- strawberry skull
- watermelon skin sign
-
animal and animal produce inspired[+][+]
- human
- mammals
- anteater nose sign
- antler sign
- batwing opacities
- bear paw sign
- beaver tail liver
- Brahma bull sign
- buffalo chest
- bull's eye sign (disambiguation)
- bunny waveform sign
- claw sign
- dog ear sign
- dog leg sign
- dromedary hump
- ears of the lynx sign
- eye of tiger sign
- feline esophagus
- giraffe pattern
- hidebound sign
- ivory phalanx
- ivory vertebra sign
- joint mouse
- leaping dolphin sign
- leopard skin sign
- moose head appearance
- panda sign
- piglet sign
- pleural mouse
- raccoon eyes sign
- rat bite erosions
- rat-tail sign
- Scottie dog sign
- Snoopy sign
- stag's antler sign
- staghorn calculus
- tiger stripe sign
-
zebra sign (disambiguation)
- zebra sign: (cerebellar hemorrhage)
- zebra spleen: arterial phase (spleen)
- zebra stripe sign (osteogenesis imperfecta)
- amphibians
- birds
- bird beak sign (disambiguation)
- bird's nest sign (lung)
- crow feet sign
- egg on a string sign
- eggshell calcification (breast)
- eggshell calcification (lymph nodes)
- gooseneck sign (endocardial cushion defect)
- gull wing appearance
- hummingbird sign
- owl eyes sign
- pooping duck sign
- sitting duck appearance
- swallowtail sign
- swan neck deformity
- winking owl sign
- fish and marine life
- reptiles
- arthropods
- micro-organisms
- fictional creatures
-
food inspired[+][+]
- Cheerio sign (disambiguation)
- chocolate cyst
- cottage loaf sign
- double Oreo cookie (glenoid labrum)
- doughnut sign (disambiguation)
- hamburger sign (spine)
- head cheese sign (lungs)
- honeycombing (lungs)
- hot cross bun sign (pons)
- ice cream cone sign (middle ear ossicles)
- ice cream cone sign (vestibular schwannoma)
- licked candy stick appearance (bones)
- linguine sign (breast implants)
- macaroni sign
- omental cake
- Oreo cookie (heart)
- pancake organ (disambiguation)
- Polo mint sign
- salad oil sign (breast implants)
- sandwich sign (disambiguation)
- sandwich vertebra
- sausage digit
- spaghetti sign
- Swiss cheese sign
-
alphabet inspired[+][+]
- A line (US artifact)
- C sign (MSK)
- delta sign (disambiguation)
- E sign
- H-shaped vertebra
- H sign
- J-shaped sella
- J sign (shoulder)
- L sign (brain)
- lambda sign (disambiguation)
- M sign
- omega epiglottis
- O sign (gastric banding)
- P sign (epiglottis)
- S sign of Golden
- tau sign
- T sign (disambiguation)
- U fibers
- U-figure (pelvis)
- U sign (brain)
- V sign (disambiguation)
- W hernia
- X-marks-the-spot sign
- Y sign (epidural lipomatosis)
- Z deformity
-
Christmas inspired
- Christmas tree bladder in neurogenic bladder
- holly leaf sign in calcified pleural plaques
- ivy sign in leptomeningeal enhancement
- nutcracker esophagus in esophageal dysmotility
- shepherd's crook deformity of the femur in fibrous dysplasia
- snowcap sign in avascular necrosis
- snowman sign (disambiguation)[+][+]
- snowstorm appearance in complete hydatidiform mole and testicular microlithiasis
- miscellaneous[+][+]





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.